
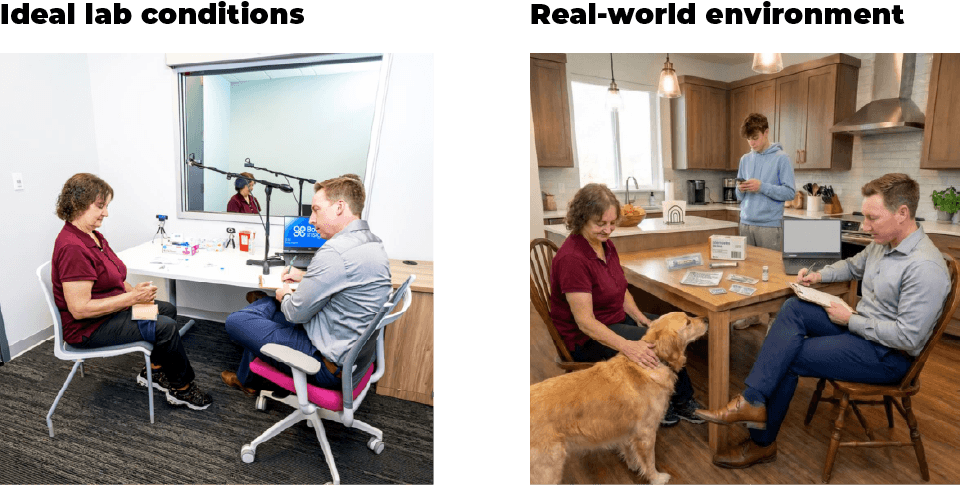
When a patient manages a chronic condition at home, they are not doing it in a clean, well-lit room with a researcher watching from behind a one-way mirror. They are doing it at 6 a.m. on a cluttered kitchen counter, distracted by kids getting ready for school.
The FDA explicitly states that to understand how a device’s design affects safety, we need to observe users in their actual use environment. But as researchers know all too well, in the lab, participants are on your time; in the home, you are on theirs. Stepping into someone’s private space presents a maze of logistical, ethical, and methodological challenges. Here are the hard truths and lessons we have learned from the field.
Finding respondents and getting in the door
The per-participant cost of in-home ethnographies can be significantly higher than that of lab studies, so you rarely have the luxury of a hefty over-recruitment approach. If you start layering overly narrow screening criteria, requiring highly specific combinations of demographics, behaviors, and environments, your participant pool shrinks so rapidly that finding an eligible person is like looking for a unicorn.
Even when you find the right people, criteria disconnects happen. We frequently see incorrect screener responses in which participants claim to use a medication or device they do not use. Because of this, consider visually confirming their device with photos or a video call during the screening process.
We also cannot underestimate the burden on participants. Standard recruitment assumes (mostly) short, structured sessions, but ethnographic participation is immersive. When participants realize the observation might unintentionally disrupt the daily routines they are trying to maintain, dropout rates can spike. To combat this, prioritize building trust before you arrive. Showing up at their door should never be your first point of contact. Leverage trusted intermediaries (like advocacy groups or clinics), conduct pre-visit intro calls, and firmly cap your sessions at 90 minutes to prevent participant fatigue.
Consent is a household affair
Consent logistics for in-home studies require a complex, multi-layered framework. You aren’t just consenting a single patient; you might encounter caregivers, adolescents, or a family member who is not directly involved in the process but is there for emotional support. An unaware teenager might wander into the room. Be ready with extras of all forms for these unexpected participants.
While you can streamline paperwork by using one primary IRB-approved adult consent form with addendums for different user groups, the ethical execution must be planned out ahead of time. For example, when relying on a caregiver for proxy consent, they must use “substituted judgment”—deciding what the patient would have wanted, not what is convenient for the study. Researchers have an obligation to watch for “implied dissent” from the patient, such as signs of distress, facial tension, or changes in breathing, which immediately overrides the caregiver’s consent. Participant safety and consent are priorities.
Micro-ethics and emotional ergonomics
Homes don’t have standard operating procedures; people do. Regardless of a home’s physical condition, participants have their own system in place. When we observe a skipped step or a bizarre workaround, we are not there to teach or train them on the “right” way to do it; our job is to uncover the “why” behind their behavior. Intervening to correct them leads to data bias and masks a systemic usability risk that the manufacturer wants and needs to see.
Once in the home, you will inevitably face the “ethnographer effect,” where participants might suddenly clean, perform competence, or hide their nonadherence simply because you walked through the door. You will also face “micro-ethics” on the fly. If a participant casually reveals a highly risky behavior, a family conflict, or active clinician nonadherence, leaving the cameras rolling can be unethical or highly distorting. In these vulnerable moments, more data is not necessarily helpful data. You must be prepared to pivot to less intrusive methods, like having the participant sketch a map or narrate an experience.
Ultimately, you have to account for the emotional ergonomics of care. Emotions like fear, shame, judgment, and fatigue aren’t just color commentary; they directly alter a patient’s risk tolerance and disclosure.

Safer devices start in the real world
The home is an unregulated care unit. Patients adapt, improvise, and develop systems that work for them, whether or not those systems match the intended manufacturer’s instructions. Ethnographic research is how medical device teams get honest about that reality. The teams that invest in this kind of field research don’t just end up with better data, they end up with safer devices.
Want to go deeper?
Bold Insight Partner Courtney Roberts recently presented Lessons from the field: Recruiting, adapting, and learning from patient ethnographies in healthcare research at the HFES International Symposium on Human Factors and Ergonomics in Health Care.